
Most content about health advocacy is written for the wrong audience. There are guides for patients learning to navigate insurance claims, courses for nursing students pursuing advocacy careers, and articles for individual advocates speaking up for their own care needs. Very little covers what is health advocacy from the organizational perspective. This guide addresses the work of nonprofits, coalitions, and cause-based groups that build campaigns to change policy and shift community health outcomes.
This guide is for the staff and directors running those organizations. It covers the definition, the types of campaigns organizations run, real examples, and the outreach methods that determine whether a campaign reaches its goals.
What is health advocacy?
Health advocacy is the effort of individuals, organizations, and coalitions to protect and improve health outcomes by mobilizing people, evidence, and resources toward policy change, expanded access, and public education.
The consensus definition, drawn from Wikipedia’s health advocacy article and WHO guidance: “Health advocacy encompasses direct service to the individual or family as well as activities that promote health and access to health care in communities and the larger public.”
Two parts of that definition are worth separating. The first is direct service: helping individuals navigate a healthcare system that is often inaccessible or confusing. The second is systems change: working to alter the policies, institutions, and social conditions that shape health outcomes for entire communities. These are not two versions of the same work. They require different skills, different stakeholders, and different organizational models.
The two levels of health advocacy
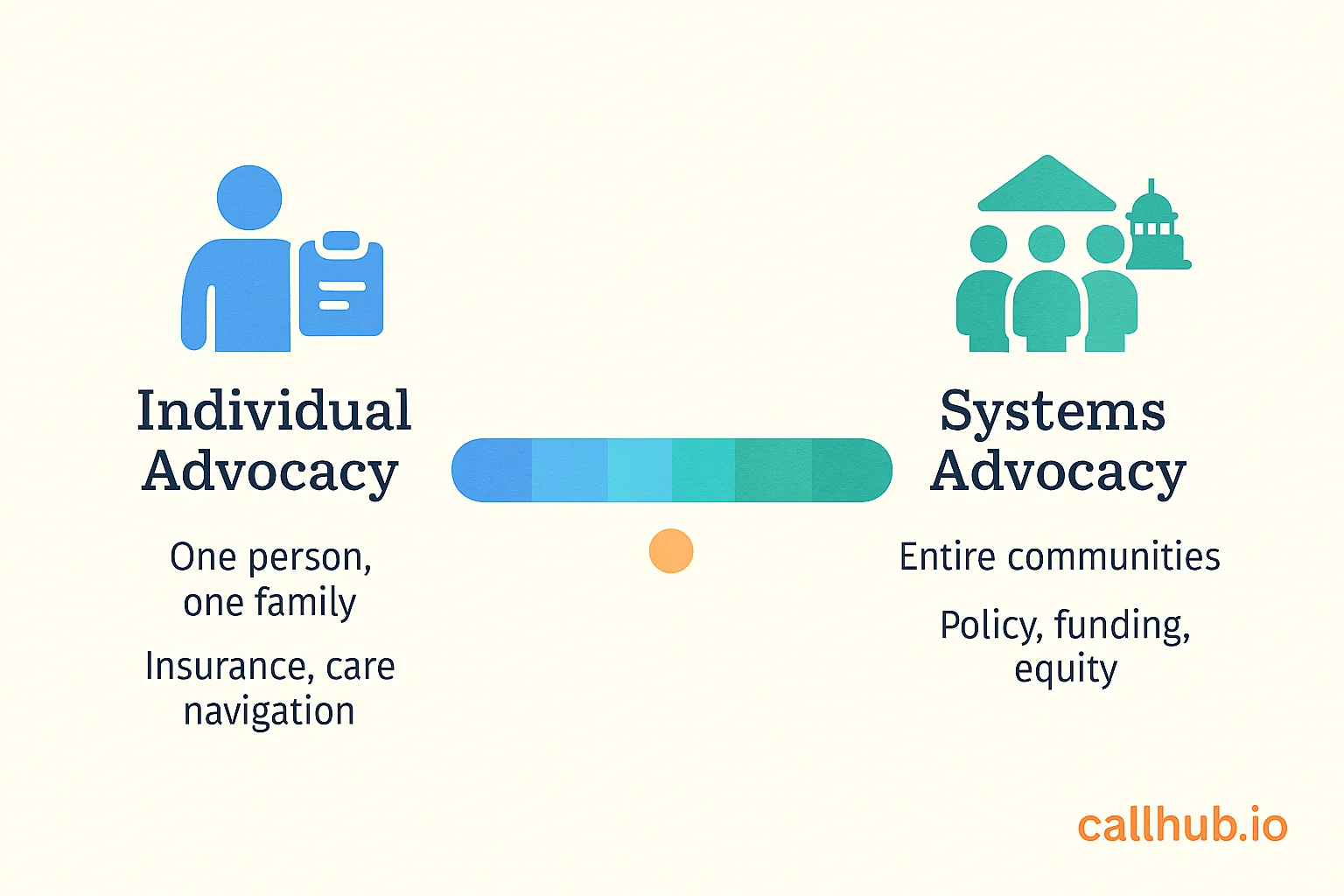
Every health advocacy effort sits somewhere on a spectrum from direct individual support to systemic policy change. Understanding where your organization operates, and where it could operate, is the starting point for designing effective campaigns.
Individual and patient advocacy: navigating the system
Individual health advocacy focuses on a specific person or family. A patient advocate helps someone understand a diagnosis, navigate insurance paperwork, appeal a coverage denial, or find appropriate specialists. This work is direct, relational, and often time-sensitive.
Organizations doing individual advocacy include hospital-based patient navigation programs, health insurance ombudsman services, and condition-specific support networks for cancer patients, rare disease families, and people managing chronic conditions.
Community and systems-level advocacy: changing the system
Community and systems-level advocacy targets the conditions that determine health outcomes across entire populations. Rather than helping one person navigate the system, it works to change the system itself.
The issues this type of advocacy addresses include Medicaid expansion, environmental regulations protecting communities from pollutants, equitable distribution of healthcare facilities, and policy frameworks addressing health disparities rooted in race, income, or geography.
Most cause-based advocacy organizations operate at this level. They are not substitutes for clinical care but organizers of the political and social conditions that make good health possible.
Types of health advocacy

Health advocacy organizations are often defined by the issue or mechanism they work on. The four most common types are disease-specific advocacy, environmental health advocacy, policy and legislative advocacy, and community health advocacy.
Disease-specific advocacy
Disease-specific organizations concentrate on a single condition or disease category: Cancer, HIV/AIDS, mental health, rare genetic conditions, and others. They combine research funding, patient support services, and policy advocacy to advance treatment access, reduce stigma, and improve outcomes for affected populations.
Organizations like the American Heart Association and the National Alliance on Mental Illness (NAMI) operate at national scale, combining public education, direct research funding, and active lobbying for policy changes that benefit their constituencies.
Environmental health advocacy
Environmental health advocacy connects environmental conditions such as air quality, water contamination, and toxic exposure to community health outcomes.
The Love Canal Homeowners Association, formed in 1978 in Niagara Falls, New York, is one of the earliest documented examples. Residents organized to document health harms from a chemical waste dump beneath their neighborhood and secured a federal emergency declaration and relocation assistance. Decades later, organizations like West Harlem Environmental Action (WE ACT) continue this work in communities disproportionately burdened by environmental hazards.
Policy and legislative advocacy
Policy advocacy targets the legislative and regulatory systems that govern healthcare access, funding, and standards. Organizations working at this level engage in testifying at legislative hearings, submitting public comments on proposed regulations, running constituent education programs, and organizing constituent contact with elected officials.
The debate over the Affordable Care Act produced organized policy advocacy at a scale rarely seen in domestic health policy. Both sides mobilized millions of constituents and thousands of organizations into a visible, coordinated campaign to influence legislative outcomes.
Community health advocacy
Community health advocacy focuses on health education, local resource access, and the social determinants of health within specific geographic communities. These organizations often work closest to the populations they serve, running peer educator programs, community health worker networks, and local outreach campaigns covering topics from vaccination to prenatal care to mental health resources.
Research published in PMC (National Institutes of Health) shows that peer educators and community health workers bring firsthand experience and credibility that increases engagement and behavior change compared to institutional outreach alone.
Examples of health advocacy in action
Four campaigns illustrate what health advocacy looks like at the organizational level:
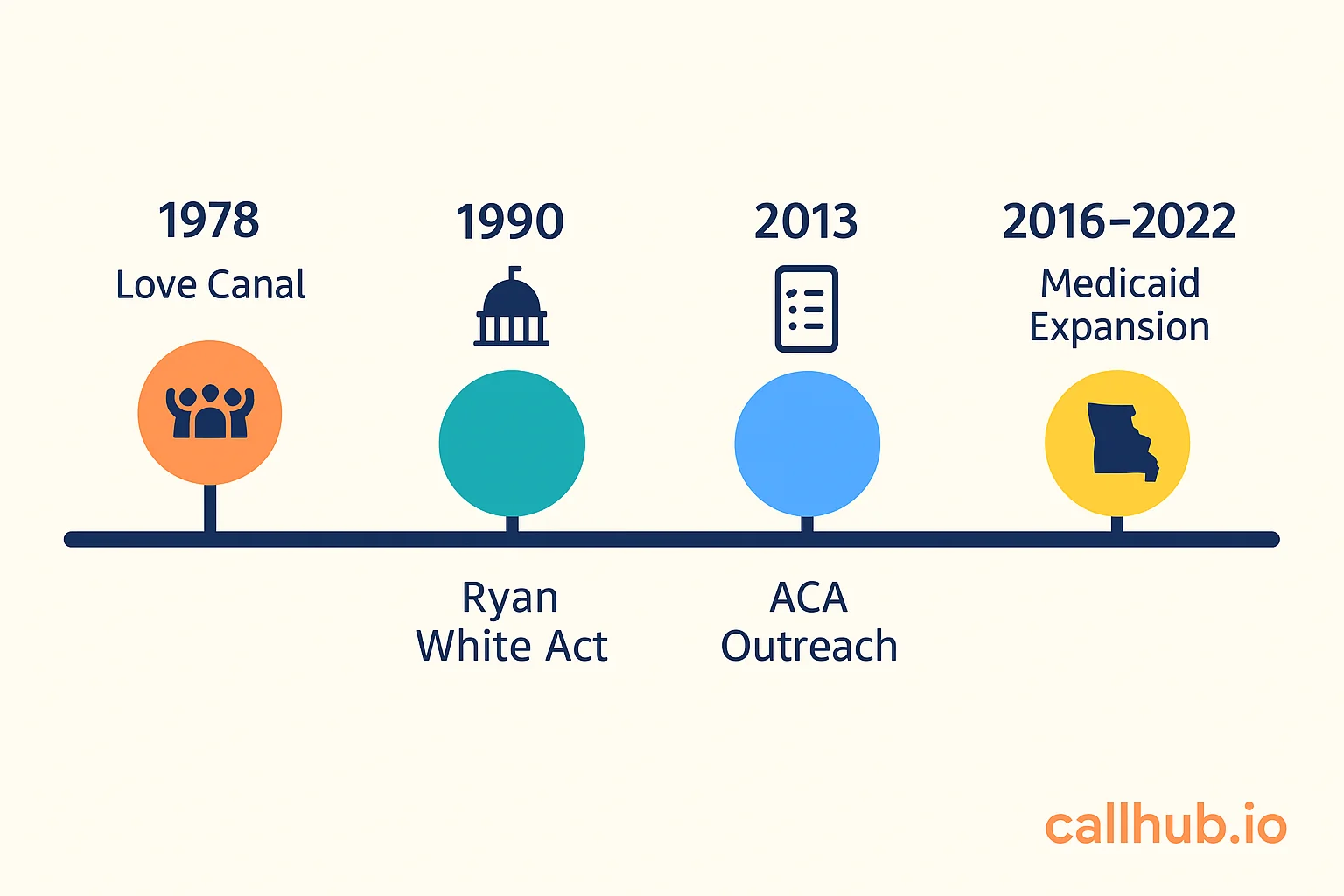
The Ryan White CARE Act (1990): Organized by AIDS advocacy groups facing a public health crisis with no federal funding framework, advocates including ACT UP and the National Association of People with AIDS mobilized congressional testimony, public protest, and media advocacy. The Act now funds care for more than half of people with HIV in the United States.
Love Canal Homeowners Association (1978): Lois Gibbs and her neighbors documented a pattern of health problems connected to chemical exposure, organized their community into a formal advocacy structure, and successfully pressured state and federal governments to respond. This campaign is studied as a foundational model of grassroots health advocacy.
ACA enrollment outreach campaigns (2013–2014): Following the ACA’s passage, a network of nonprofit organizations ran coordinated campaigns combining in-person enrollment events, peer-to-peer texting, and phone outreach to reach uninsured populations. These campaigns used multi-channel outreach to reach communities where standard broadcast methods fell short.
State Medicaid expansion ballot campaigns: In states where Medicaid expansion required ballot approval, health advocacy coalitions ran organized constituent contact programs. Montana, Oklahoma, Missouri, and South Dakota all passed Medicaid expansion through ballot initiatives that advocacy coalitions helped qualify and win.
How organizations run health advocacy campaigns
Building a campaign that generates constituent engagement, reaches policymakers, and produces measurable impact requires an organizational model, not just a message.
Building a supporter and volunteer base
Every health advocacy campaign depends on a base of people who care enough to take action. Building that base is not a pre-campaign activity. It is the campaign.
Effective supporter base-building includes:
- Constituent recruitment through community events and partner organizations: Identify the populations most affected by the issue and create low-barrier entry points such as signing a petition, attending an information session, or joining a text list
- Peer educator and ambassador programs: Recruit supporters with personal experience of the health issue and train them to engage their own networks. PMC research confirms that peer educators produce higher engagement than organizational outreach alone
- Tiered engagement pathways: Move supporters from passive (following updates) to active (making calls or attending hearings) through structured escalation. Ask for small commitments first, then larger ones as trust builds
- Data hygiene from the start: Collect name, phone, email, and location at every touchpoint. A disorganized contact list cannot be activated at scale
Multi-channel outreach: calls, texts, and in-person
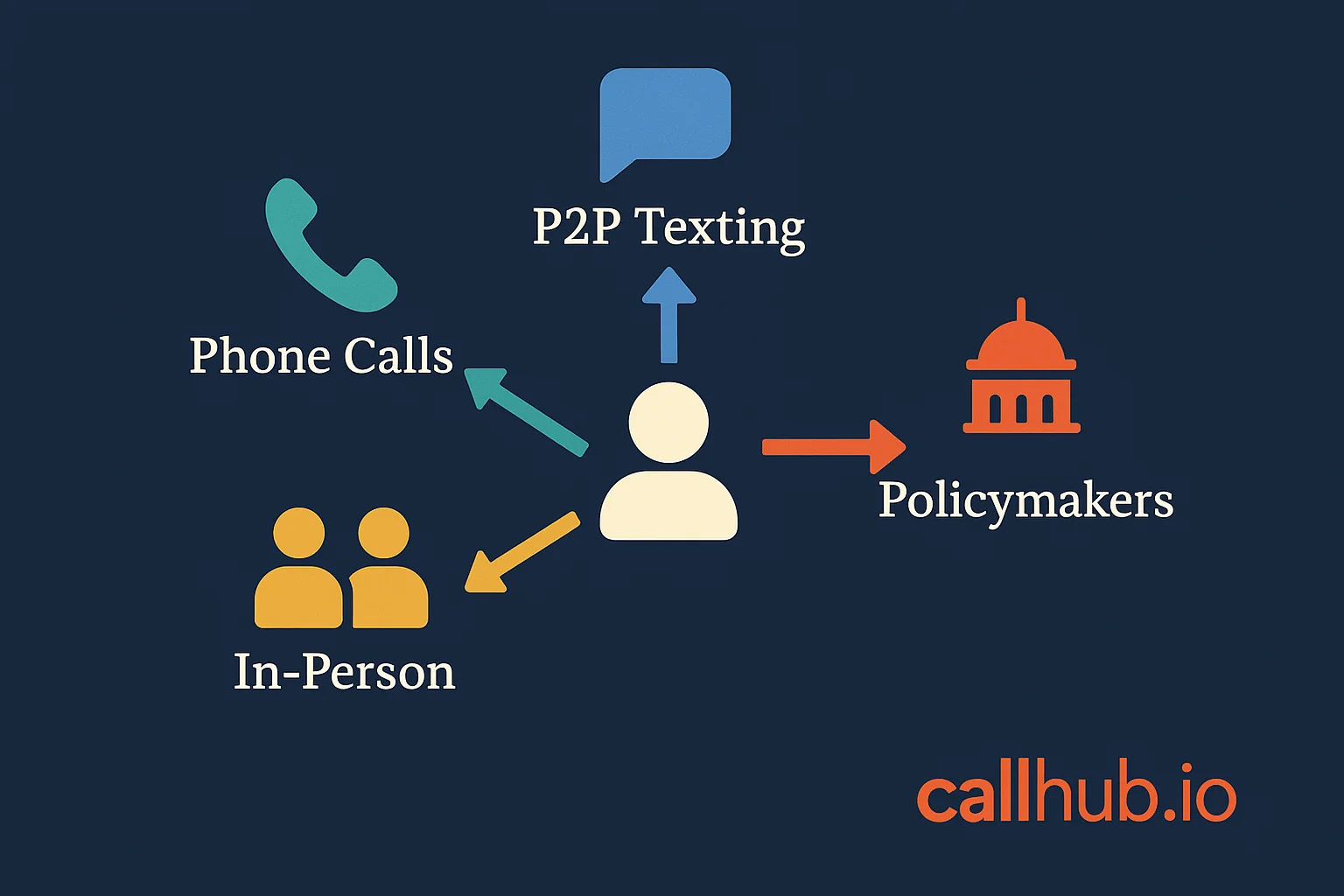
Reaching supporters and policy targets effectively requires matching the channel to the goal.
Phone calls are best for high-stakes constituent contact: getting supporters to call their legislators, conducting intake interviews with affected community members, or running mobilization programs before a legislative vote or hearing. A live volunteer call creates a social commitment that a mass email does not.
Peer-to-peer texting (P2P texting) works best for information sharing, event invitations, and short action asks with supporters who have already opted in. Shannon Goecke, Communications Specialist with the National Union of Healthcare Workers (NUHW), notes what text tracking adds: “Unlike email, you can’t really track open rates and click rates on text messages. But with the URL tracker, you can. I love that function.”
In-person outreach at community health fairs, enrollment events, town halls, and partner organization visits creates the trust and relationship depth that digital channels cannot replicate, particularly in communities with lower digital access.
Public health communications research from Marymount University confirms that multi-channel strategies spanning digital platforms, community media, and in-person outreach ensure health information reaches diverse audiences where they are. No single channel reaches everyone.
For organizations ready to scale outreach calls, phone banking tools for advocacy organizations and secure text messaging for healthcare organizations cover the tool setup. For a full walkthrough of volunteer calling programs at the nonprofit level, phone banking for nonprofits and grassroots outreach covers the structure from list setup to outcome tracking.
Policy and legislative engagement
Connecting constituent outreach to specific policy asks is what separates advocacy campaigns from general awareness work. Effective policy engagement includes:
- Direct constituent contact programs: Organized calls and texts from constituents to their elected officials on a specific bill or regulatory comment period
- Testimony coordination: Recruiting and preparing constituents to testify at committee hearings or public meetings
- Legislative meetings: Scheduling and preparing supporters for in-person meetings with legislators or their staff
- Public comment campaigns: Mobilizing constituents to submit comments during regulatory notice periods. The FTC, HHS, and EPA all rely on public comment processes that organized campaigns can influence at scale
The connection between constituent contact volume and legislative response is direct. Most legislative offices track call and meeting volume on specific issues, and a campaign generating 200 constituent contacts in two weeks creates a signal that staff will pass to the member.
Measuring advocacy impact
Health advocacy organizations often find it difficult to measure whether their work is making a difference. The metrics that matter depend on the campaign phase:
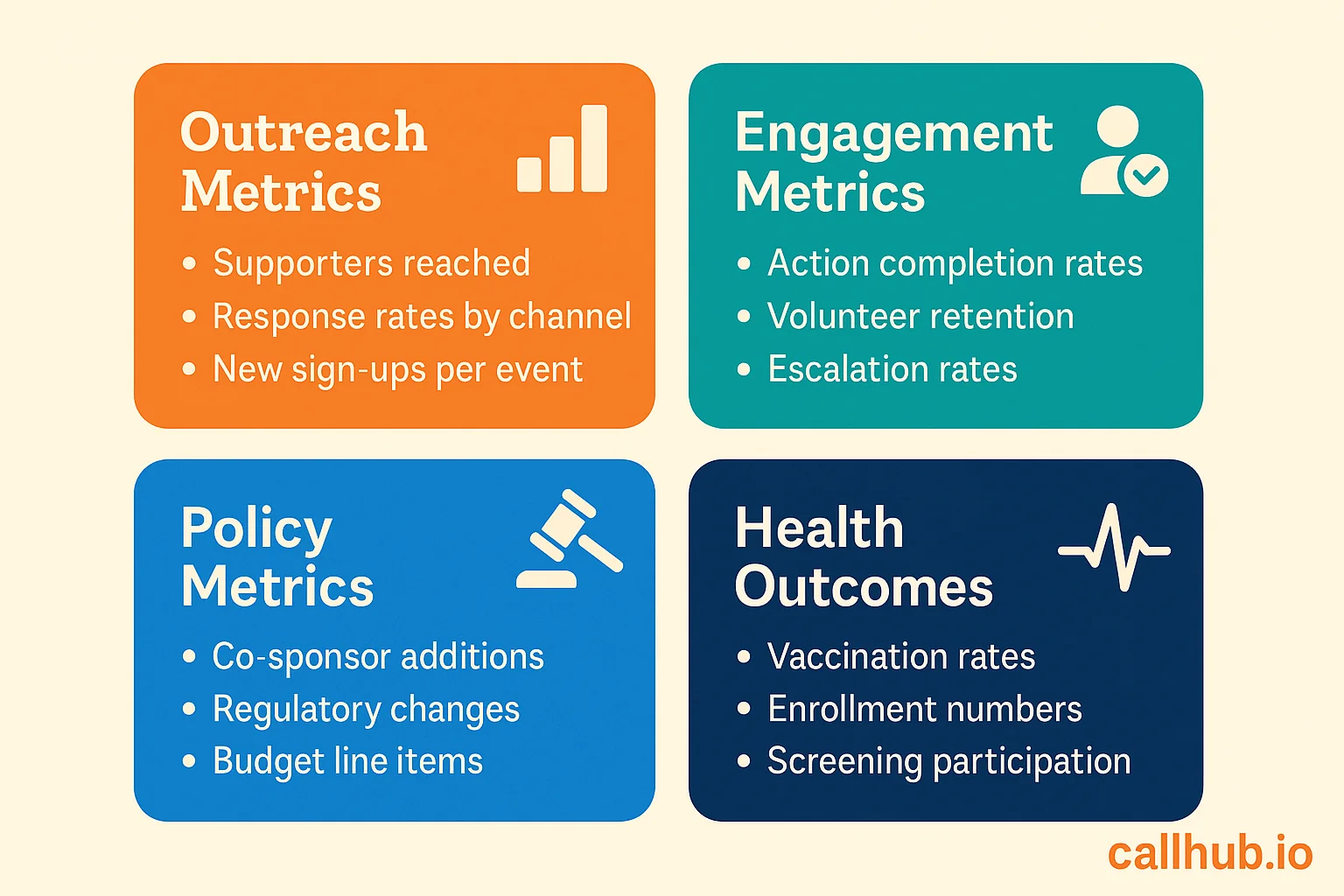
- Outreach metrics: Number of supporters reached, response rates by channel, new sign-ups per event or campaign
- Engagement metrics: Action completion rates (calls made, letters sent, testimony submitted), volunteer retention and escalation rates
- Policy metrics: Bill co-sponsor additions, regulatory changes, budget line items added or protected
- Health outcome metrics: For community-level campaigns, longer-term measures like vaccination rates, enrollment numbers, or screening participation in the target community
Start with what you can track: Outreach volume and action completion rates. Build toward policy and outcome measurement as the campaign matures.
Why health advocacy matters: the outcomes
Health advocacy produces changes that individual clinical care cannot. The healthcare system addresses the patient in front of it. Health advocacy addresses the conditions that determine whether people can access care, afford it, and receive it in a form that meets their needs.
Three categories of outcomes demonstrate this:
Policy change: The Ryan White CARE Act, Medicaid expansion across 14 states, and environmental regulations protecting communities from industrial pollution are direct outcomes of organized advocacy campaigns. Without organized constituent pressure, none would have happened on the same timeline.
Expanded access: Community health outreach campaigns that connect uninsured populations with coverage options, vaccination programs that reach communities with historically low uptake, and patient navigation programs that help people access care they’re already entitled to all produce measurable outcomes in enrollment, vaccination rates, and healthcare utilization.
Health equity: The intersection of health advocacy with racial and economic justice is not incidental. It is structural. Most health advocacy organizations working at the community level specifically target the populations that existing health systems underserve. Campaigns designed to address that gap produce measurable changes in outcomes for communities that clinical care alone has not reached.
For organizations building the fundraising infrastructure that makes advocacy campaigns sustainable, the 501c3 fundraising rules and compliance guide covers the legal framework governing nonprofit advocacy activities and funding sources.
Ready to run your first health advocacy campaign?
Health advocacy is one of the few mechanisms that can change the conditions that determine health outcomes at scale. Organizations that combine a clear policy goal, a mobilized base of supporters, and multi-channel outreach (calls, texts, and in-person contact working toward a shared target) consistently outperform those treating advocacy as a communications activity rather than an organizing one.
The next step after understanding the landscape is building the campaign itself. See how nonprofits and advocacy organizations design and run campaigns that move policy: Healthcare Advocacy: How to Run Campaigns That Work
Frequently asked questions
Who can be a health advocate?
Anyone can act as a health advocate, but the role looks different depending on context. At the individual level, patients, family members, and trained patient navigators advocate for access to care, coverage, and appropriate treatment. At the organizational level, nonprofit staff, community health workers, and policy specialists run campaigns targeting systemic health conditions. Some states license or certify professional health advocates for clinical navigation roles, but most community and policy advocacy work does not require licensure.
What is the difference between patient advocacy and public health advocacy?
Patient advocacy focuses on a specific individual. It helps them navigate care, understand options, and access services. Public health advocacy targets the systems and policies that determine health outcomes across entire populations. A patient advocate helps someone appeal an insurance denial. A public health advocate campaigns for the policy change that would reduce insurance denials system-wide. The two are complementary: Individual advocacy surfaces what system-level advocacy should target.
How do you become a health advocate?
There is no single credential for health advocacy work. Patient advocates typically come from clinical backgrounds such as nursing, social work, or care coordination, and may pursue professional certifications through the Patient Advocate Foundation or similar organizations. Community health advocates and nonprofit staff more often come from organizing, public health, social work, or directly from the communities they serve. Many advocacy organizations prefer direct community experience and a track record of organizing over formal credentials.
What are the most common health advocacy issues?
Current major issue areas include access to mental health care, prescription drug pricing and affordability, Medicaid expansion and coverage gaps, environmental health impacts on lower-income and minority communities, reproductive health policy, public health funding and workforce capacity, and chronic disease management support. The most active areas shift by legislative cycle and public health context, but access, affordability, and equity run through most of them.
How do health advocacy organizations fund their work?
Most health advocacy organizations fund their work through a combination of foundation grants, individual donors, government grants (for service-focused organizations), and member dues (for coalition models). 501(c)(3) nonprofits can fund advocacy and public education but face restrictions on direct electoral activities. 501(c)(4) organizations can engage in more direct political advocacy. Understanding which activities are allowable under each structure is essential before building a campaign budget. See the 501c3 fundraising rules and compliance guide for the relevant legal framework.
What tools do health advocacy organizations use for outreach?
For constituent outreach and campaign mobilization, health advocacy organizations use contact management systems (CRM), phone banking platforms for volunteer-driven calling programs, peer-to-peer texting platforms for personalized outreach, and email systems for mass communication. Organizations running legislative contact campaigns also use patch-through calling systems that connect constituents directly to their elected officials. Outreach tools should feed back to a central database, whether that is Salesforce, EveryAction, or NationBuilder, so supporter data stays current across channels without manual import/export.


