


In 1999, nurse advocacy in California produced something historic. The California Nurses Association coordinated years of bedside insight, hospital by hospital, into a sustained legislative campaign. The result: California Assembly Bill 394, the first law in the United States to mandate nurse-to-patient staffing ratios.
That campaign didn’t start in Sacramento. It started at the bedside, with nurses recognizing a pattern that individual patients couldn’t see and no single administrator would acknowledge. According to the Gallup Honesty and Ethics poll, nurses have held the most trusted profession ranking in the United States for 22 consecutive years. The California nurses turned that trust into constituent pressure.
Most nurse advocacy stays at the bedside, protecting one patient at a time. This article is about what happens when it doesn’t, and how you run the campaign.
What nurse advocacy means
Nurse advocacy is the practice of acting on behalf of patients and the healthcare conditions that affect them. It operates at two levels: The individual level, where a nurse protects one patient’s rights within the current system, and the systemic level, where nurses work to change the policies and structures that create patient harm across a population.
The two levels are not alternatives. Most working nurses practice both. But they require different skills, different tactics, and different scales of organization.
Nurse advocacy is the practice by which nurses act as representatives and defenders of their patients, both at the bedside and in the broader healthcare policy environment. It encompasses direct patient protection, informed consent facilitation, and organized efforts to reform the policies and systems that shape patient outcomes at scale.
Bedside advocacy: Protecting each patient in your care
At the bedside level, nurse advocacy means speaking up when a patient’s treatment plan doesn’t align with what they want, what they understand, or what is safe. It means translating clinical information into plain language, flagging missed consent, and escalating concerns about care quality through the right channels.
This form of patient advocacy in nursing is constant and immediate. It doesn’t require a campaign. It requires the willingness to speak, and the knowledge of when your voice carries weight.
Research published in BMC Nursing identifies the primary barriers to bedside advocacy: Workload, institutional hierarchy, fear of retaliation, and lack of managerial support. These aren’t abstract constraints. They’re the reason systemic advocacy matters: When individual nurses can’t speak up inside the institution, the only path is changing the institution itself.
Systemic advocacy: Changing the conditions patients live with
Systemic advocacy operates outside the ward. It’s the work of influencing legislation, regulation, and policy that determines how healthcare is delivered, funded, and structured. It’s where individual cases become population-level data, and where bedside insight carries its highest value.
A nurse who has seen five patients turned away from mental health care in one month holds evidence that no researcher can replicate. When that nurse contacts a state senator’s office and describes what they’ve witnessed firsthand, it carries weight that a policy brief cannot.
This is the level that requires organizing. And organizing requires tactics.
The patient rights advocate’s core responsibilities
The role of a nurse patient advocate covers six core responsibilities:
- Informed consent: Ensuring patients understand the procedures, risks, and alternatives before agreeing to treatment.
- Care translation: Converting clinical language into terms the patient can act on.
- Complaint and grievance navigation: Helping patients escalate concerns through the right institutional channels.
- Treatment plan alignment: Verifying the care delivered matches the care the patient actually chose.
- Discharge safety: Confirming patients have safe and realistic discharge plans before they leave the facility.
- Rights documentation: Recording instances where patient rights were raised, how they were addressed, and what follow-up occurred.

These responsibilities position the nurse as the patient’s most reliable check in a system that’s designed for throughput, not personalization. They’re also how nurses accumulate the observational data that powers systemic advocacy campaigns.
Why nurses are unusually credible systemic advocates
The numbers are straightforward. The U.S. Bureau of Labor Statistics counts 4.3 million nurses in the United States, making nursing the largest single healthcare workforce. That’s more potential constituent contacts than any lobbying firm can generate.
But volume isn’t the whole story. The Gallup trust ranking matters in a specific way: Constituent credibility. When a nurse contacts a legislator’s office, the staffer on the other end of the line knows this isn’t a hired advocate. A registered nurse carries a professional identity organized entirely around patient care, and that framing is unusually difficult to dismiss.
Nurses also hold frontline evidence that policy analysts simply can’t replicate. Policy proposals are often abstract. Nurses make them concrete. “Here’s what this regulation does to this type of patient, in this unit, at this frequency” is a different argument than a white paper, and legislators know it.
Step 1: Pick a specific, winnable advocacy target
The most common mistake in nurse advocacy campaigns is starting too broad. “Improve healthcare” is not an advocacy target. “Pass SB-242, which would require minimum staffing ratios in emergency departments, before the May session ends” is.
Your advocacy target needs three things: A specific policy ask, a decision-maker who has actual authority over it, and a realistic timeline to a decision.
Translate a patient problem into a policy ask
Start with a pattern, not a single case. One incident may be isolated. Three to five similar incidents suggest a systemic problem. Ten suggest a policy gap.
Ask yourself: What would have to change at a policy level to prevent this from happening to the next patient? The answer, stated as a specific, actionable request, is your policy ask. “Require hospitals to disclose nurse-to-patient ratios publicly” is a policy ask. “Better staffing” is not.
Match the ask to the right decision-maker
Different advocacy targets have different decision-makers. Getting this wrong wastes campaign resources and your coalition’s credibility.
| Ask type | Decision-maker |
|---|---|
| Staffing ratios, scope of practice | State legislature, state nursing board |
| Reimbursement rules, Medicare and Medicaid coverage | Federal legislature, Centers for Medicare and Medicaid Services (CMS) |
| Hospital-level policies | Hospital administration, board of directors |
| Licensing rules | State nursing board |
| Workplace safety standards | Occupational Safety and Health Administration (OSHA), hospital HR |
A state senator cannot set Medicare reimbursement rates. An OSHA complaint cannot change scope-of-practice law. Identify the correct decision-maker before you run a single outreach call.
Step 2: Build your coalition
Nurse advocacy campaigns rarely win on nursing constituent contacts alone. The strongest campaigns combine the nursing workforce with patient advocacy groups, allied health professionals, and community organizations that share an interest in the outcome.
Start with nurses and allied health workers in your unit
Your first coalition is the people you already work with. A floor of 20 nurses who each agree to contact their state representative during a specific 72-hour window generates 20 constituent calls in one news cycle. That’s visible to legislative staff.
Allied health workers, including respiratory therapists, physical therapists, and social workers, often face the same policy constraints you do. They’re natural coalition partners who expand both your constituent count and your professional credibility on the issue.
Join your state nursing association’s advocacy network
Every state has a State Nurses Association affiliated with the American Nurses Association (ANA). These organizations have existing relationships with legislators, established advocacy networks, and infrastructure for mobilizing nurses around specific legislative campaigns.
Their advocacy networks are the most efficient on-ramp to systemic advocacy for individual nurses. You’re not building from zero. You’re joining infrastructure that already knows how to move constituent contacts at scale.
The full breakdown of types of advocacy explains how coalition-building tactics differ by advocacy type. Nurse advocacy campaigns typically combine legislative advocacy (contacting elected officials) with organizational advocacy (pushing healthcare systems internally). Understanding which mode you’re in affects who you recruit and how you deploy them.
Connect with patient rights organizations
Patient rights organizations bring something your nursing coalition can’t: The patient’s own voice. Their members are often motivated to contact legislators precisely because they’ve been personally affected by the policy you’re trying to change. And constituent contacts from patients carry a different emotional weight than contacts from professionals.
Search for patient rights organizations aligned with your specific issue: Disease-specific nonprofits, hospital patient advocacy groups, and consumer health rights coalitions. The advocacy software guide for nonprofits is a useful resource for coalition partners who are new to outreach tools and need to get up to speed quickly.

Step 3: Run your outreach campaign
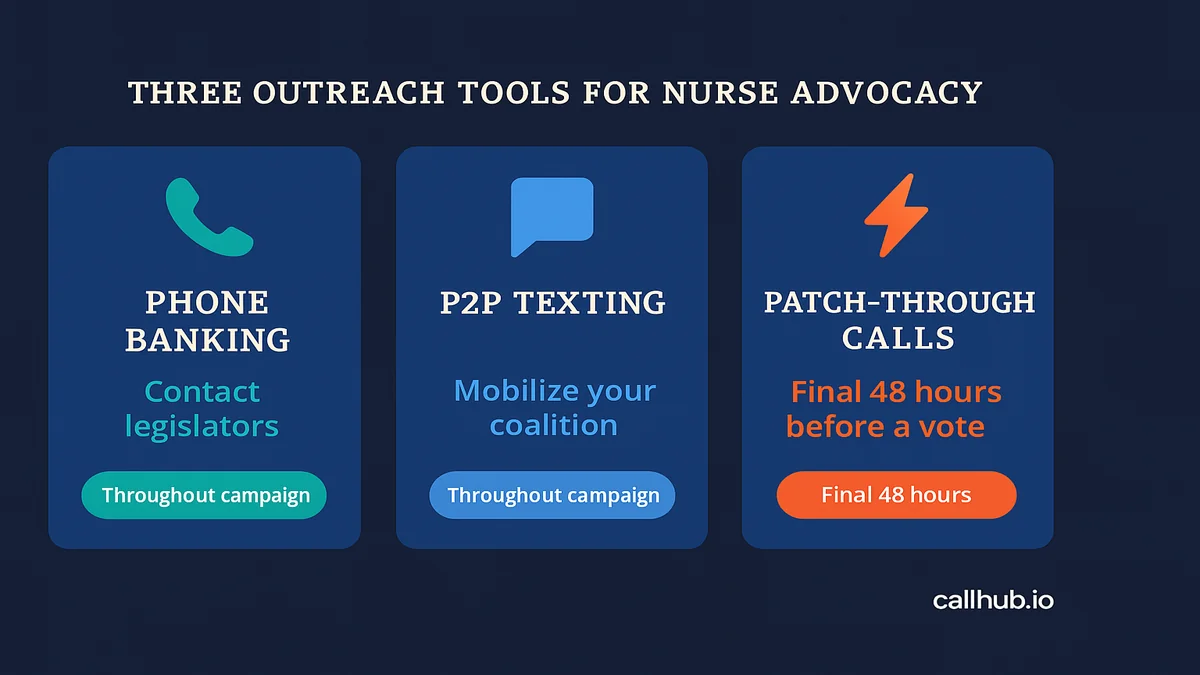
The outreach phase is where constituent pressure becomes concrete and measurable. Three tools carry most of the weight in a nurse advocacy legislative campaign: Phone banking, peer-to-peer texting, and patch-through calling.
Phone banking to legislators: Registering constituent volume
Legislative staff track constituent contact volume. When a nurse calls her state senator’s office and identifies as a constituent, that call is logged. The Analyst Institute documents that call volume to a legislator’s office is a key signal staffers use to gauge constituent priority, which directly shapes how the legislator prioritizes committee votes.
This is why volume matters. A call from one nurse is a data point. A hundred calls from nurses across a district, within a 48-hour window, is a priority signal.
Phone banking software for advocacy campaigns makes this scalable. Volunteers log in, receive a contact queue, follow a script, and log call outcomes in real time. The campaign manager sees live response rates and can redirect volunteer time mid-session toward legislators who are still undecided.
Effective phone scripts for nurse advocacy calls are short: 30 to 45 seconds. State who you are (registered nurse, name of hospital or unit), what you’re calling about (the bill number and what it does for patients), and what you’re asking for (a yes vote, a meeting, support for a specific amendment).
No reading from paper. No multi-minute monologues. Legislative staff handle high call volume and appreciate brevity.
Peer-to-peer texting to mobilize your nurse network
Phone banking works for outbound contact to legislators. Peer-to-peer texting works for mobilizing your own coalition, specifically for getting nurses to take action during a critical window.
Peer-to-peer texting (P2P texting) means each message is sent individually by a real person and arrives as a personal text, not a mass broadcast. Response rates are significantly higher than email, and the medium creates an expectation of a genuine two-way exchange.
Use it to send a colleague the sample call script and ask if they can make three calls tonight. Use it to share a live floor vote link and ask coalition members to contact their rep right now. Use it to follow up with nurses who received the ask but haven’t yet acted.
Patch-through calls when the vote is imminent
A patch-through call connects a constituent directly to a legislator’s office in real time, eliminating the steps of finding a number, dialing, and navigating a voicemail system. When a floor vote is within 24 to 48 hours, Patch-through Calling can move significant constituent contact volume in a compressed window.
It works this way: A nurse volunteer calls into your campaign line, hears a brief prompt about the bill, and is immediately connected to their state representative’s office. They speak directly to staff. The call is logged as a constituent contact from that district.
Use Patch-through Calling as a high-urgency, final-window tactic, not as a routine outreach method throughout a campaign.
Step 4: Track progress and sustain pressure
Advocacy campaigns that don’t track outcomes lose momentum between peaks. Progress tracking keeps your coalition motivated and your strategy calibrated to where pressure is actually needed.
| What to track | Why it matters |
|---|---|
| Total constituent contacts made | Baseline for measuring mobilization |
| Contacts per legislator, per district | Shows where pressure is concentrated or thin |
| Legislator position changes | Evidence that the campaign is moving votes |
| Coalition size over time | Indicates whether recruitment is growing or stalling |
| Media mentions of your issue | Signal of issue salience to legislators |
Sustaining pressure across a legislative session requires cycling tactics. Phone banking creates volume. Peer-to-peer texting maintains engagement between peaks. Meeting requests and editorial board letters build credibility in the longer arc between votes.
Most advocacy campaigns win not through a single dramatic moment but through sustained, documented constituent presence across the legislative calendar.
Nurse advocacy in practice: Three campaigns that worked
California staffing ratios: From bedside to state law
California’s nurse-to-patient ratio campaign ran for years before AB 394 passed in 1999. The California Nurses Association organized nurses unit by unit, collected incident documentation across hospitals, and built a legislative strategy around the weight of documented patient harm.
The key to the California campaign was specificity. The nurses didn’t argue that staffing was generally inadequate. They argued for a specific number: One nurse to five patients in medical-surgical units, one to two in intensive care. Specific asks are passable into law. General complaints are not.
This is the policy advocacy guide for nonprofits and campaigns framework applied directly: A specific target, a coalition of nurses and patient groups, sustained constituent contact, and documented engagement over multiple legislative sessions.
Telehealth access: Nurses pushing for rural patient coverage
After the pandemic expanded telehealth coverage under emergency orders, advocacy campaigns in multiple states pushed to make those expansions permanent. Nurses in rural areas were central to those campaigns because they had direct evidence of what telehealth access had done for their patients: Fewer missed appointments, earlier interventions, and measurably better chronic disease management.
The coalition structure followed the same pattern: Identify the specific policy at risk (sunset provisions in state telehealth bills), build a coalition of rural health providers and patient organizations, and generate constituent contacts with the relevant legislators before the session closed.
The coalition’s value was the patient voice alongside the professional credibility. Nurses provided authority and documentation. Patient groups provided personal testimony and emotional weight. Both were necessary to move the votes.
A national union’s legislative calling drive
National Nurses United has coordinated legislative calling campaigns around federal staffing legislation. The model: Identify nurses in the congressional districts of specific House and Senate committee members, mobilize them to call during the markup period, and document the contact volume to both the office and the press.
The tactic relies on geography. A nurse calling her own representative’s office carries more weight than a nurse calling from outside the district. The campaign’s infrastructure identifies which coalition members live in which district, then routes outreach accordingly. Volume from the right districts is what moves a committee vote.
The policy gap only a nurse can close
Nurses hold the most direct, documented evidence of what healthcare policy does to real patients. No policy analyst, no lobbyist, and no administrator accumulates the same observational depth across a patient population. That evidence only becomes policy change when it’s organized.
The complete guide to health advocacy for healthcare organizations covers the broader framework for healthcare advocacy programs. For the outreach component of your campaign, phone banking software for advocacy campaigns gives you the infrastructure to turn your coalition’s constituent contacts into measurable legislative pressure.
The gap between what nurses know and what policy reflects is real. Closing it requires organizing.
Frequently asked questions
What is nurse advocacy?
Nurse advocacy is the practice of acting on behalf of patients and the healthcare conditions that affect them, at both the individual and systemic level. At the bedside, it means protecting individual patient rights and ensuring informed consent. At the systemic level, it means organizing campaigns to change the policies and structures that affect patient populations.
What does a nurse patient advocate do?
A nurse patient advocate performs six core functions: Ensuring informed consent, translating clinical information into accessible language, helping patients navigate complaints and grievances, verifying treatment plan alignment, confirming safe discharge plans, and documenting instances where patient rights were raised or contested.
What is the difference between bedside advocacy and systemic nursing advocacy?
Bedside advocacy protects individual patients within the current healthcare system. Systemic advocacy, also called patient advocacy nursing at scale, works to change the system itself through legislative campaigns, policy reform, and organized constituent outreach. Both forms are part of nurse advocacy, and most working nurses practice both throughout their careers.
What are the barriers to nursing advocacy?
Research published in BMC Nursing identifies four primary barriers: Workload (leaving no time for advocacy beyond the immediate shift), institutional hierarchy (making it difficult to challenge physicians or administrators), fear of retaliation (discouraging individual nurses from speaking up), and lack of managerial support (removing the organizational backing necessary for sustained advocacy). Systemic advocacy through external campaigns often sidesteps these internal barriers entirely.
How can nurses influence health policy?
Nurses influence health policy by organizing constituent contact campaigns targeted at specific legislation or regulatory decisions. The most effective tools are direct legislator contact through phone banking, peer-to-peer texting outreach to mobilize the nursing network, and Patch-through Calling during high-stakes votes. Coalition-building with patient groups and allied health professionals amplifies the constituent count and the diversity of voices reaching the decision-maker.
What is the difference between nurse advocacy and lobbying?
Lobbying is a specific legal category of advocacy that involves direct attempts to influence legislation, often by paid professionals representing organized interests. Nurse advocacy can include lobbying activities (contacting legislators, testifying at hearings), but it also includes activities outside the legal definition: Public education, media engagement, and community organizing. Individual nurses engaging in advocacy as private citizens are not subject to lobbying disclosure requirements.
How do nurses organize patient advocacy campaigns?
Nurses organize advocacy campaigns by identifying a specific policy target, building a coalition of nurses, allied health workers, and patient groups, and running structured outreach to decision-makers during the legislative window. The practical steps: Pick a winnable, specific ask; identify the decision-maker who controls it; recruit coalition members from your unit, your state nursing association, and aligned patient organizations; brief them on the outreach script; deploy phone banking and peer-to-peer texting during the critical window; track contact volume by district; and sustain pressure through the vote.


